Unit 6 Study Guide Review Module 15 Surface Area and Volume of Solids Answer Key
![]()
Evaluation of an Electronic Medical Tape Module for Nursing Documentation in Paediatric Palliative Care: Interest of Nurses with a Think-Aloud Arroyo
by one,*  , 1,ii , ane , 2,3 , 2,iii , 4 , two,3,5 and 1
, 1,ii , ane , 2,3 , 2,iii , 4 , two,3,5 and 1
1
Section of Didactics and Educational Inquiry in Wellness Science, Kinesthesia of Health, Witten/Herdecke University, 58448 Witten, Germany
2
PedScience Research Institute, 45711 Datteln, Federal republic of germany
three
Section of Children's Pain Therapy and Pediatric Palliative Care, Kinesthesia of Health, School of Medicine, Witten/Herdecke University, 58448 Witten, Germany
4
Smart-Q Softwaresystems GmbH, Lise-Meitner-Allee 4, 44801 Bochum, Germany
five
Pediatric Palliative Care Centre, Children's and Adolescents' Infirmary, 45711 Datteln, Germany
*
Author to whom correspondence should be addressed.
Academic Editor: Ziad El-Khatib
Received: 6 February 2022 / Revised: four March 2022 / Accepted: fourteen March 2022 / Published: 18 March 2022
Abstract
Background: Paediatric palliative intendance (PPC) is a noncurative approach to the care of children and adolescents with life-limiting and life-threatening illnesses. Electronic medical records (EMRs) play an important role in documenting such complex processes. Despite their benefits, they can introduce unintended consequences if future users are not involved in their development. Aim: The aim of this study was to evaluate the acceptance of a novel module for nursing documentation past nurses working in the context of PPC. Methods: An observational report employing concurrent think-aloud and semi-structured qualitative interviews were conducted with 11 nurses working in PPC. Based on the main determinants of the unified theory of credence and use of engineering science (UTAUT), information were analysed using qualitative content assay. Results: The main determinants of UTAUT were constitute to potentially influence credence of the novel module. Participants perceived the module to exist cocky-explanatory and intuitive. Some adaptations, such as the reduction of fragmentation in the display, the optimization of disruptive mouseover fields, and the use of familiar nursing terminology, are reasonable means of increasing software adoption. Conclusions: After adaptation of the modules based on the results, further evaluation with the participation of future users is required.
1. Introduction
Paediatric palliative care (PPC) (for acronyms see Appendix A) is a multidisciplinary and noncurative approach to the care of children and adolescents with life-limiting and life-threatening illnesses [1,two,3]. Approximately 21 million children are in demand of PPC [four]. The conditions of patients undergoing PPC are oftentimes rare [5], complex, and range from neuromuscular [half dozen] to genetic and congenital diseases [2]. In general, oncological diseases account for a smaller proportion of this total [7]. The aim of PPC is to provide psychosocial, physical, and spiritual back up to children and their relatives [viii], and to manage symptoms such every bit pain and impairment in communication [9]. Patients experiencing PPC undergo numerous admissions and discharges to and from inpatient and outpatient settings over the course of their lives [10]. To overcome the resulting fragmentation of wellness care systems, major challenges be in the coordination of treatment and care [eleven].
The complex care and treatment of patients in PPC is reflected in loftier demands for documentation [12]. In detail, electronic medical records (EMRs) play an increasingly important function in PPC for documenting complex processes [11,12,13]. These records tin facilitate communication among multiple professions [xiv] and support care coordination and planning [eleven]. In clinical practice, EMRs accept numerous advantages in terms of providing different functions, such equally access to patients' data in real time, sharing information with other providers, and recording reminders and alerts [15]. EMRs tin can potentially increase the overall quality of care and time efficiency [xvi].
Nurses play an important function in PPC, as they are responsible for providing intendance and support for the afflicted patients and their relatives [17]. They are i of the major user groups for EMRs [18], and they spend a large proportion of their working time on documentation [19]. Although nurses generally express a positive attitude towards digital documentation [twenty], the introduction of EMRs tin be accompanied by negative perceptions [21,22,23] and unintended consequences [24,25]. In the literature, consequent results are constitute for different countries [26,27,28]. For case, poor usability of EMRs has a negative impact on the wellbeing of nurses [29], and can produce stress and frustration [xxx] or cognitive failure [eighteen]. Additionally, this cistron is associated with burnout [28]. Similar results tin can also be identified for physicians as users of EMRs [31,32]. In different studies, nurses also tend to have a negative perception of spending more time on digital documentation than with patients [29].
To prevent such negative consequences of EMRs, it is necessary to involve nurses in the development of EMRs by using a participatory design process [33,34] to ensure that EMRs are context sensitive [35]. This process entails that EMRs and their functions must be adjusted to the clinical context in which they are used. If this requirement is not considered, the implementation of EMRs can interrupt nurses' usual ways of thinking and workflows, and thus atomic number 82 to additional documentation work [21,36,37]. A participatory design process encompasses the interest of users in a process of artistic development, which is characterized by four main principles [34]: (one) democratization of decision-making processes; (2) common learning processes; (3) observation of latent (tacit) knowledge structures; and (iv) mutual inventiveness through collaborative work amidst developers, researchers, and (time to come) users. This arroyo is a prerequisite to ensure that work processes and usability are considered during development [38] and remain a factor for the success of the implementation of EMRs [39].
It is relevant to apply a theoretical perspective of technology acceptance when carrying out participatory development for new technologies. Theories and models from acceptance inquiry are used here, such as the "unified theory of acceptance and use of engineering (UTAUT)" [40,41]. UTAUT includes four key straight determinants of behavioural intention to utilise a engineering from the user perspective: performance expectancy, endeavor expectancy, social influence, and facilitating conditions [40,41]. In the context of acceptance inquiry on EMRs, UTAUT is equally applicative [42,43].
This report is a role of the ELSA-PP project, which aims to adapt an EMR from adult care to inpatient settings that provide PPC. In this project, requirements for an EMR in the context of PPC were collected, and different modules were programmed [44]. For example, a novel patient chart module has already been evaluated with the participation of physicians and nurses [45].
Enquiry question: How do potential future users in the context of inpatient PPC perceive the module for nursing documentation in terms of engineering credence, and what are their wishes for improvement of the module?
The aim of this report was to evaluate the acceptance of a module for nursing documentation for the inpatient setting of a PPC unit from the perspective of potential users in the context of PPC and to involve those users in the development process.
two. Materials and Methods
2.1. Study Design
For the evaluation of the module for nursing documentation, a qualitative observational study was conducted in September 2022 over a period of three weeks. The method of concurrent thinking aloud (CTA) was combined with a subsequent qualitative interview [46]. With CTA, cerebral processes and reasons for user actions tin can be assessed while interacting with a engineering [47]. In the context of a task-oriented arroyo, participants were asked to perform everyday tasks of nursing documentation using the novel module and to verbalize their thoughts while doing so [46,48]. In usability testing of new technologies, CTA is the near frequently used method [49], and it is also used in participatory design [33].
The ideals committee of Witten/Herdecke Academy obtained upstanding blessing for this study (approval code: 35/2019).
2.two. Participants and Recruitment
Nurses from a PPC unit of a children'southward and adolescents' hospital in Germany were asked to participate in this study. Posters and flyers were distributed to provide information about the study'south aim and procedure. In addition, reminders were given during shift changes at the PPC unit. Further written informational fabric and a consent grade were handed out if nurses expressed an involvement in participating. Financial compensation of €twoscore for taking part in the report was offered. At this PPC unit, the participants are documenting the bulk of their clinical documentation in paper-based records.
two.3. Information collection and Testing Procedure
To ensure equally much participant flexibility as possible, two options were provided for the testing process: (one) remote and (2) contiguous. In both options, two researchers were present at near every session, with one conducting the interview and one writing field notes. The procedure for data collection was otherwise identical for both options. Audio and screen movements were recorded as a screencast using the software Captura (version 8.0) in both cases.
- (1)
-
Remote testing: During remote sessions, participants shared their screen with evaluators using the software Zoom. Relevant documents were sent to participants in advance by email.
- (ii)
-
Face-to-face testing: Face-to-face testing sessions were conducted in a regular office shut to the PPC unit of measurement, with the evaluators using a standardized software and hardware setup. The hardware setup consisted of a computer with a mirrored screen then that the researchers could detect the use of the modules.
At the get-go of each session, participants were informed about the aims and methodical procedure of the study. From previous studies in the ELSA-PP project, near of the nurses in the PPC department of the children'south and adolescents' hospital were already familiar with the procedure [45,50]. Within the task-oriented framework, the tasks served to structure the CTA and were presented in printed class. Participants were instructed kickoff to read all tasks aloud and were encouraged to enunciate all thoughts while performing the tasks. Participants were informed that the researcher would remind them to think-aloud if they ceased verbalizing their thoughts [46]. This approach is recommended when using the CTA method, because participants reducing or completely ceasing verbalization after some time is a known behaviour [51]. To reduce discomfort among participants, they were told that there was "no right or wrong" in testing, and that the aim of the report was non to exam them, but to test the module [51]. The modules were filled with exemplary dummy information concerning a fictional patient to stimulate the thinking of the participants.
For this study, after the completion of the tasks, an exploratory and open up approach was chosen to discuss solutions with the participants in the spirit of participatory pattern [49]. Yet, during the functioning of the tasks and the duration of thinking aloud, interaction with the participants was kept to a minimum to reduce bias [46]. Participants were brash that if they encountered issues when using the modules, they should showtime expect for a solution themselves. However, they could ask for assist at whatsoever time. For this purpose, standardized questions for problem solving were formulated to reduce bias due to the influence of the researchers (Appendix B) [51].
A semi-structured interview guide was developed through discussion and a concluding process of consensus building by the researchers. The questions were related to general impressions of using the modules as well as to aspects of usability, comprehensibility, and time to come wishes for further evolution (Appendix C).
2.4. Module for Nursing Documentation
The module for nursing documentation consists of three components in which nursing activities tin can exist documented: (I) nursing care, (2) wound care, and (III) nursing care planning (Figure 1). The components were adult as function of the ELSA-PP projection and were integrated into the software Information-System Palliative Intendance (ISPC) (company: smart-Q, Germany), which is used for adult palliative intendance. The module does non include sure aspects of documentation, such as vital signs, symptoms, or wake−sleep rhythm, which were the discipline of a previous study in which a patient nautical chart module was evaluated [45].
two.five. Data Analysis
Audio files were transcribed verbatim following the unproblematic rules developed by Dresing and Pehl, and were transferred to MAXQDA (2020) alongside related videos [52]. The assay was carried out independently by two researchers (S.K. and T.Southward.B.). First, all statements and observations were assigned to the tasks and were annotated with the relevant screen movements. Later, these statements and observations were deductively assigned to the primal determinants of the UTAUT, which serve every bit the main category (Table 1). Later on, inductive subcategories were formed. This procedure resulted in a coding system, which was finalized through discussion and consensus edifice (50.A.D. and C.J.). Quotations were translated into English language and assigned a pseudonym (ID) (Nurse_transcript-ID_#timecode#).
3. Results
Testing sessions were conducted with eleven female nurses (Table 2), including 7 face-to-face sessions and four remote sessions. Session duration ranged from 43 min to 97 min, with an average of 56 min.
In full, 499 codes were assigned within the coding system, with a range of 35 to threescore codes and an average of 45 codes per interview. Due to the large number of observations and statements, only especially pregnant categories with the largest number of codes are reported beneath. Three chief categories were formed, (I) performance expectancies, (Two) effort expectancies, and (III) facilitating conditions, with a total of 16 subcategories (Figure ii). No codes could exist assigned to the UTAUT determinant social influence.
3.ane. Performance Expectancies
This theme includes all topics regarding "the degree to which an private believes that using the arrangement will aid him or her to accomplish gains in task functioning" [41], which encompasses mainly the functionalities of a technology based on UTAUT.
-
(a) Self-explanatory and like shooting fish in a barrel-to-use
As a general impression, participants perceived all iii modules as cocky-explanatory and piece of cake-to-use. This impression was often complemented past verbalizations that they basically had to become accustomed to the awarding.
"Well, in itself I call up it is quite skilful and also as detailed equally information technology is now described here, always quite self-explanatory. But I call back it is however quite difficult at start, because it is merely a change, and at the beginning, we volition merely click on different things, I think, to look for where it is really to exist constitute in the end or where I tin can enter something exactly once again."
(Nurse_01_#01:12:15#)
-
(b) Support and time reduction through checkboxes
Participants perceived the use of checkboxes in all components to be practical and useful. This characteristic was peculiarly discussed past many participants in the documentation of wound care, as the documentation of wounds was often perceived to be time-consuming. Here, examples were highlighted when complex wounds needed to be treated, such equally in patients with epidermolysis bullosa.
"But I think if you really have such patients [with decubiti], or we merely have a patient with, for example, epidermolysis bullosa, where yous besides have to alter the dressing every two days, it is quite practical if you just have to mark a [predefined] list with a cantankerous [the checkbox] concerning what the wound is cleaned with and what information technology is fixed with and what kind of materials are used. Because otherwise, it is a lot of piece of work to keep lists and write things downward."
(Nurse_06_#00:29:23#)
-
(c) Usefulness of the to-exercise function
In general, the to-practice function in the components concerning wound care and nursing care planning were perceived to be useful in supporting nursing care. Here, the ability to ascertain tasks for the nurse'due south own piece of work, as well equally assigning tasks to other colleagues, was described as useful. The use of this function was also seen every bit a ways of facilitating communication with other professions, e.g., when working with physicians.
In addition, it was desired in this context that the to-do lists could be grouped individually. For case, if a nurse is looking subsequently three patients, information technology should be possible to display only the to-do lists for these patients.
"Then, I think that is really good. And that I tin and so maybe as well select times, then, I would like to select that a physician is coming to the next intendance. Because the doctors would then probably also meet that it is a to-do for them. And I do not accept to run later them and say, 'Remember, you lot take to come to modify the dressings or something else'. I think that is definitely very, very good."
(Nurse_01_#00:51:43#)
-
(d) Calculation context-specific information with gratuitous text fields
In all three components, participants requested the power to enter contextual information past adding free text fields. For example, in the documentation of nursing activities, a free text field was requested to add data apropos the specific materials that were used in nursing care. Furthermore, a complimentary text field was requested for the clarification of wounds, as at that place were only checkboxes with predefined terms for the description of wounds.
- Nurse:
- "Can I add together additional information somewhere, so that everyone [colleagues] also knows, aha, the pare must be creamed with the cream XY and non with wound protection cream?".
- Interviewer:
- "Is it not intended yet, merely you would just wish that 1 could insert data here every bit free text?".
- B:
- "Yes, for instance. We ofttimes write additional data in the [paper-based] nursing documentation, and that corresponds a bit to the intendance planning here. That you then see: Aha, we are now using cream XY or water only. I would miss that hither now." (Nurse_09_#00:ten:51#).
-
(e) Restoration of issues in nursing care planning from by hospitalizations
When documenting the nursing intendance plan, participants requested that problems from by hospitalizations exist restored from the archive as current bug. The rationale for this request was that patients undergoing PPC are often readmitted as the disease progresses, and the bug of such patients are ofttimes seen again in the context of new hospitalizations. Here, it was considered a work-saving measure for bug not to accept to be redefined and re-described in their entirety.
"Yes, I would like that. So, if the nursing problems are transferred to the archive, if the patient was already here in May [in the PPC unit], I say, and the patient comes dorsum now and I can really accept over one-half of the problems i to ane, because information technology has not changed. For instance, if the patient still tends towards constipation or still has secretion bug, you still do the same thing, that y'all can quite simply just click, and information technology [the software] takes over automatically."
(Nurse_08_#01:19:08#)
-
(f) Usefulness of the trunk scheme for wound documentation
The participants particularly emphasized that they found the body scheme helpful in marking wounds. They ofttimes described this process as being more than precise and quicker to draw than the performance of the same task on paper.
"Oh yes, it works. Exactly, I retrieve it is skilful that yous have such a scheme, such a torso scheme. Because sometimes you cannot describe it as well as you might have seen it, i.due east., where the spot is. So, I think that is bully. Exactly, here I can enter everything with five centimetres, two centimetres, whatever."
(Nurse_08_#00:32:25-7#)
3.2. Attempt Expectancies
This theme includes all topics regarding "the degree of ease associated with the use of the system" [41], and basically includes the dimension of perceived usability and complexity of use.
-
(a) Fragmentation of the brandish
The participants perceived a fragmentation of the display in the component for documenting nursing activities. When documenting nursing activities, the fact that the heading (Headline in Figure 3) was moved out of the field when scrolling downwards was institute to be impractical.
"What I find a fleck impractical when I scroll downward is that y'all and so no longer meet the headline: then have to whorl upward again and then I come across which nursing activity I accept to click on. And where did I end upwardly at present?"
(Nurse_08_#00:08:29#)
-
(b) Visibility of functions
In the component for documenting nursing activities, participants were not able to identify how nursing activities should be documented. This upshot was attributed to the fact that the checkboxes that had to exist clicked to document the nursing activities were not visually raised. The checkboxes were greyed out, as were the headings. Therefore, a large percentage of participants became irritated, which led to a longer search for the function (checkboxes).
"If I click on that now? Tin you do that? No. […] Only you cannot click on that now? […] Well, this is all hither non to click on, no. I find that irritating now, because I do not know how to do document the nursing activities."
(Nurse_03_#00:04:05#)
-
(c) Employ of familiar nursing terminology
In the component for documenting nursing activities, the free text field for documenting the nursing report was non recognized every bit such by the participants. This upshot was specially the consequence of the fact that the gratuitous text field was labelled "comment" and did not use the specific phrase "nursing report"; nevertheless, some participants saw and named the field annotate directly.
- Nurse:
- "Okay, in the nursing written report, in the free text, I take to certificate a nursing report. It is up there at present. Just looking. […]. Cannot add together it here, tin I? Oh, perhaps in the filed 'comments'".
- Interviewer:
- "But I could add some costless text at that place now. Just you would not take recognized it as such now, so to speak?".
- Nurse:
- "I would not have recognized it [the field 'comments' for 'nursing report']".
- Interviewer:
- "What would help yous recognize that sooner?".
- Nurse:
- "I retrieve that would actually have to exist called nursing report too." (Nurse_03_#00:09:38#).
-
(d) Confusing mouseover field
For nurses to be able to runway which activities have been documented, all documentations are transferred to the patient chart view (Effigy iv). The patient chart view is the center of the EMR, where physicians and nurses document, due east.g., vital signs, sleep patterns, symptom observations, or notes on catheter direction. When presenting documented nursing activities in the patient chart view, the mouseover field in which the activities were presented after saving the documentation was perceived to exist disruptive (Figure 4).
"I find that [the mouseover field] totally confusing here. If I click on information technology now, it shows me what I accept done [which activities were documented]. I notice that super disruptive. I wouldnot exist able to cope with it, I would give up again."
(Nurse_09_#00:32:08#)
three.3. Facilitating Conditions
This theme includes all themes regarding "the degree to which an individual believes that an organizational and technical infrastructure exists to support use of the system" [41].
-
(a) Bereft number of reckoner workstations
Concerns were described that after the implementation of digital documentation with EMR, an bereft number of estimator workstations would be available. This situation could create conflicts, considering non all nurses would be able to document at the same time.
"That we do not accept enough workstations with computers. That one wants information technology, the side by side and there, that there is friction, exactly. Yes, that would exist one of the biggest fears I have."
(Nurse_11_#00:46:12#)
-
(b) Fears concerning technical bug
Fears apropos technical bug were frequently expressed. In particular, fears concerning losing an internet connection or a full general system crash were described. In particular, concerns were described about not being able to access patient information, such as information regarding medications, in an emergency.
"That information technology does not work and I cannot access the electronic medical record. That would requite me a stomach-ache, that I just could not go to the things that were important for the patient correct now. That I do not know, okay, now I do no know, the patient is cramping, I need a medication now, but I practise non know what I can give because I cannot admission the electronic medical record. Or what if the internet fourth dimension is non working or the connection is just too tedious."
(Nurse_09_#01:xxx:08#)
-
(c) Near-bedside documentation
In addition, from the participants' perspective, it would be useful if documentation could be carried out near the bedside of the patient. This location for documentation was perceived to be easier because the nurses practise non have to call up the contents of the nursing documentation or accept to write them down on a piece of paper by hand. In the latter case, they have to document this information at a workstation abroad from the bedside.
"But otherwise with the implementation [of the EMR], is it meant that nosotros so have it [the EMR] on a tablet, so we could take it with usa [to the patient'due south room]? Because I think that if you take information technology with you, you can do it direct later on you take done something [eastward.k., nursing activities] with the child. Or whether you lot must become dorsum [to a workstation] again get-go."
(Nurse_08_#00:56:09#)
-
(d) Efficiency and readability
In addition, participants expressed the hope that digital documentation would increase the efficiency of nurses' work by eliminating the burden of handwritten documentation. In this context, it was also noted that readability is increased by digital documentation, as handwriting is often difficult to read.
"I am hoping that once you are well into information technology [the digital documentation] and y'all know where to enter what, that information technology will not take as much fourth dimension as the handwritten documentation. That, and maybe also that you exercise non accept to write anymore so much [by paw]. That it is all easy to read, above all, even the doctor'due south handwriting. And that information technology is partly too clearly shorter, more meaty […]."
(Nurse_03_#01:00:15#)
-
(east) Increased clarity of to-do lists and the assurance that things are not forgotten
Moreover, the hope was mentioned that EMR would make information technology less probable for nursing activities to be forgotten, as the EMR would provide a to-do function. As such, EMR provides automated reminders of what nursing activities yet need to be completed.
"In the long run, I hope that it will brand my work easier […]. That it is clear what you have to exercise. That the to-dos pop up in such a way that I likewise forget fewer things in the end or simply that fewer things get lost. Perchance also a little chip that things that are sometimes considered unnecessary in certain situations, that they are then extra penetratingly annoying with the to-do popular-ups and so that y'all merely practise information technology and yous do non forget information technology anymore."
(Nurse_01_#01:00:15#)
-
(f) Changeover to digital documentation hard for older users
From the participants' point of view, the transition to digital documentation would exist more than difficult for older nurses than for younger nurses (due east.chiliad., due to depression digital competencies). Nevertheless, participants were as well confident that older caregivers would exist able to cope with the transition after a period of familiarization.
"I call back that [change to] digital documentation volition be more difficult for some older colleagues, but I recall that if yous put your heed to it a bit and you go used to it, they would exist able to do information technology quite well, and I have to be prepared for it."
(Nurse_05_#00:46:17#)
four. Word
The aim of this study was to evaluate the acceptance of a module for nursing documentation for the inpatient setting of a PPC unit from the perspective of potential users involved in PPC, and to involve those users in the development procedure.
In summary, participants perceived the module to be cocky-explanatory and intuitive. In particular, a reduction in documentation workload was frequently associated with the application of the module in EMR. Based on the results identified in this study, themes are discussed that can be assessed as specially relevant for future blueprint and further development of the module and the EMR itself.
In the main category of performance expectancies, various functions were identified that were considered to be specially helpful to the participants in clinical work.
In this report, assigning tasks with the to-practice function was perceived as useful, specially in the components focused on wound care and nursing care planning. In addition to making work easier and reminding nurses of tasks to be completed, this function was also seen as helpful for interprofessional collaboration with physicians. According to the current literature, ane of the key functions of EMR for nurses is to communicate with other professionals and to structure patient care [37]. For this purpose, auxiliary functions such as instant messaging and task management software can back up interprofessional collaboration [53].
Even though the to-do role has been perceived as helpful, its awarding also poses dangers, which are a risk in clinical do. If such functions are used, for example, to assign tasks to physicians, those physicians volition receive a message for each job assigned. Consequently, the processing of such electronic messages must be done past physicians, which tin atomic number 82 to an additional burden on top of numerous other messages [54]. The processing of such electronic messages poses the take chances of an boosted brunt for physicians, who are known to bear major burdens [55]. This state of affairs tin can lead to work-related frustration. I study suggested that the management of letters may be linked to the development of exhaustion in physicians [56]. For this reason, the utilize of this role should be planned and coordinated interprofessionally, both during farther development and during implementation.
Moreover, in this written report and in other studies, ane of the master perceived benefits of using EMRs was an increment in piece of work efficiency, equally EMR utilise was viewed equally saving time spent on documentation [14,57]. In this report, the use of checkboxes and defined lists was institute to be peculiarly helpful and to make the work of caregivers easier. Although, on the i paw, the use of such features seems useful, such use is also accompanied by concerns. For case, in a qualitative study of nurses' views on the impact of EMRs, the use of checkboxes and lists was viewed critically [58]. Nurses in that report expressed concern that the apply of checkboxes, predefined dropdown menus, or cut-and-paste functions express nurses' critical thinking and that nurses who used such functions would unlearn how to think "exterior the box".
One manner of documenting content "outside the box" is to use free text fields. This functionality was requested past many participants in this written report in society to add contextual information to specific content documented using predefined lists and checkboxes. Although adding free text is important to be able to certificate specific content, using costless text fields as well often can besides be dangerous. For example, ane report institute that the use of free text fields led to a kind of "information overflow" among users due to the large amount of text to exist read [59]. It should therefore be carefully considered what sorts of content makes it necessary to use free text fields, and it is also of import to place the situations in which information technology is necessary to utilise checkboxes or predefined lists. This dilemma should be considered when implementing EMR in the context of PPC prior to implementation, and requires farther critical reflection hereafter.
In the main category of effort expectancies, information technology was too possible to place the factors that play a special part in the further development and accommodation of EMRs to positively influence acceptance.
In particular, the fragmentation of the display in the component of nursing documentation was perceived by nurses as an area in need of improvement. Fragmentation of the display is a phenomenon that is often found in the apply of EMRs [48]. The fragmentation of the display leads to users having to memorize content and consequently requires them to scroll back and forth to bring information together. In addition to full general workload, this difficulty also places an boosted mental load on the user [32]. This sociotechnical variable is also referred to equally cerebral load [60]. Therefore, ane strategy for optimizing the modules is to reduce fragmentation of the brandish. For example, a freeze function in the module for documenting nursing activities could exist used in this case to make a heading visible in the display at all times, so that users do not accept to remember the contents of this heading.
The facilitating weather identified here potentially contribute to the development of an implementation strategy for the EMR module in the context of PPC. For example, an bereft number of computer workstations was a concern highlighted past participants. Consistent with the evidence, limited access to or a express number of computers is oftentimes mentioned as a barrier to the implementation of EMRs in general [14]. Therefore, for possible implementation, the concrete requirements of hardware equipment must be considered.
Also, it is important to address fears concerning technical problems prior to implementation. In this context, nurses and physicians, also as other users, need to exist trained to bargain with technical problems in clinical do. For instance, questions need to be answered concerning how technical support can exist provided in an emergency. Insufficient technical support is as well highlighted past a scoping review on barriers to the adoption and apply of EMRs [14].
Furthermore, concerns were voiced by participants regarding how older nurses would manage the transition from handwritten to digital documentation due to their potentially low digital competencies. These concerns are consistent with bear witness from other studies on the effects of the implementation and use of EMRs for older nurses compared to their younger counterparts [21]. For case, a report conducted in an intensive care unit of measurement found that nurses' age was negatively associated with perceptions that the use of EMRs interfered with the direct care of patients and did not increase work efficiency [29]. Here, older nurses expressed their belief that the time spent on digital documentation was inadequate compared to fourth dimension spent on patient care [29]. Therefore, learning weather and learning needs must be adapted to these user groups. The content of the grooming must be oriented to their daily work processes and must include the ability to learn on the job. Similarly, digital training and learning environments should be provided [61]. However, bereft training for the use of EMRs is considered to be a major barrier for EMR adoption in general [14]. Therefore, regardless of specific training concepts for older users, sufficient training of all users is also necessary, which can increment the quality of documentation [62].
It is also relevant to interpret the results of this study from a sociotechnical perspective. For case, care in the context of PPCs is multidisciplinary in nature [8]. Thus, under everyday clinical weather, EMRs are used by nurses in interactions with other professional groups, such as physicians and social workers. A recent review of the furnishings of the implementation of EMRs has shown that EMRs can both better and worsen communication [xiv]. Consequently, the touch on of the modules evaluated here on advice with other wellness professionals in the context of PPC should be considered by further steps of the evaluation.
For the farther evolution of the modules and the EMR itself, it is necessary to first implement the factors identified hither, which can potentially influence acceptance. After, these adjustments need to exist re-evaluated by conducting further iterations with users. Post-obit this re-evaluation, consideration should also be given to the task of complementing the evaluation by other methodological approaches that are suitable for later on phases of the EMR evolution process. Here, later sufficient consideration of users' needs, expert-based methods such as heuristic evaluation or cognitive walkthroughs should be applied [48]. Other methodological approaches that simulate clinical situations should also be considered, such as "near alive clinical simulations" (NLCS), in which actors pretend to care for existent patients so as to provide a more realistic awarding scenario for evaluation [63].
In the estimation of results, it should exist considered that in this report, but individual modules of EMR were evaluated. Under clinical conditions, the application takes place while nurses collaborate with multiple modules and functions of EMRs [45]. Future evaluations should ensure that interaction with additional modules of EMR is evaluated.
Furthermore, the sample in the study could be considered sufficient to achieve data saturation. In this context, there is some discussion in the literature concerning the required sample size, especially when analysing the usability of new technologies. Drawing on the literature concerning usability assay, eighty% of all usability issues can be identified past five users [64]. In general, it is recommended to perform several iteration cycles with fewer participants instead of testing many users directly [65].
Despite the methodological limitations inherent to the application of the CTA method, the post-obit points must be noted. The CTA method makes it possible to analyse and appraise the cognitive processes of users during the execution of tasks, which provides valuable insights into users' mental models [66]. Furthermore, user actions and reactions, as well as verbalizations, tin can be assessed and recorded simultaneously, which provides valuable and rich data for the redesign of technologies according to users' needs. When the formative evaluations of the modules are completed, quantitative evaluation procedures should be used to focus specifically on the assay of usability and chore performance. Here, a retrospective think-aloud approach is recommended [67].
5. Limitations
The results obtained here must be assessed in light of the applied methodology [47]. During the utilise of the CTA method, the presence of observational evaluators may have influenced participant behaviour and verbalization (the Hawthorne Effect) [68]. It can be assumed that some participants may have formulated their statements more positively or suppressed negative statements due to social desirability [63]. Nevertheless, it cannot be excluded that the results, respectively the behaviour and the statements of the participants, are biased due to social desirability [64].
Moreover, in add-on to the application of the software itself, the CTA method also affects the cognitive load of participants, as they must concentrate on performing tasks and verbalizing simultaneously [47]. The resulting dual cognitive load may have influenced the completeness of the verbalized information [68]. This cistron probably also influenced the participants' perceptions of their cognitive load after the awarding of the modules. It is also hypothesized that participants' simultaneous focus on task performance and verbalization may lead to incomplete information [69]. This incompleteness results from the fact that, due to cognitive focusing, participants forget to study other important information.
Moreover, it must exist considered that CTA was applied under laboratory conditions during a short application flow. Information technology must exist causeless that the results may differ in everyday practice under stressful clinical situations [65]. In improver, it is likely that farther needs volition be verbalized by users during longer-term use of the modules in clinical practice. This fact must be taken into consideration given the sociotechnical nature of EMRs. In full general, EMRs are non considered static [70], nor are hospitals or the knowledge and competences of nurses [65]. This situation ways that because of the dynamic sociotechnical environment of wellness care, continuous adaptation of the software volition be required. This requirement applies even after further iterations and even after the implementation of the evaluated modules [71]. As a natural outcome, on the one hand, the results presented provide a profound basis for understanding potential factors concerning credence and the general needs of digital documentation in PPC from the perspective of nurses. On the other hand, those elements change over time and require user-driven optimization [72].
Finally, it must exist mentioned that the results obtained here relate to the context of use in the German language health care system. Information technology is likely that in dissimilar countries, other requirements are relevant.
half-dozen. Conclusions
This written report identified factors that may have a positive impact on user acceptance. These results were obtained by effectively involving potential users in the development procedure. Overall, participants perceived the novel modules for nursing documentation as intuitive and cocky-explanatory.
In further development, the wishes of users should be implemented, and special attention should be given to reducing information overload and brandish fragmentation. Further iterations of the evaluation should be conducted with users by simulating real clinical conditions.
Writer Contributions
Conceptualization, S.K.; methodology, South.One thousand. and T.South.B.; formal analysis, S.K., T.South.B., C.J. and L.A.D.; writing—original typhoon grooming, S.Grand.; review and editing, T.S.B., C.J., 50.A.D., D.One thousand., J.P.E., B.Z. and D.Z.; visualization, S.1000.; investigation T.Southward.B., C.J., L.A.D. and S.K.; supervision, B.Z. and J.P.E.; realization of software, D.Z. and smart-Q software systems. Funding conquering, B.Z., J.P.E. and D.Z. All authors have read and agreed to the published version of the manuscript.
Funding
The enquiry in this article was funded by the European Regional Development Fund (ERDF), grant number EFRE-0801385.
Institutional Review Board Argument
This study was conducted in accordance with the guidelines of the Announcement of Helsinki and was approved by the ethics committee of Witten/Herdecke University (approval lawmaking: 35/2019), fifteen Apr 2019.
Informed Consent Argument
Informed consent was obtained from all subjects involved in the written report.
Data Availability Statement
The corresponding datasets are available from the corresponding writer upon reasonable asking.
Conflicts of Interest
After completion of the projection ELSA-PP, D.Z. (smart-Q Software Systems GmbH) will receive product rights to the software. This fact has not influenced the behave of this study.
Appendix A. Acronyms
| PPC | Paediatric palliative care |
| UTAUT | Unified theory of acceptance and use of engineering science |
| EMRs | Electronic medical records |
| CTA | Concurrent thinking aloud |
| ISPC | Information-system palliative care |
| NLCS | Near alive clinical simulations |
Appendix B. Interview Guide
Questions during the session to solve issues:
- –
-
Can y'all describe to me in your own words the problem you are having right now?
- –
-
What would you await here?
- –
-
What would you have expected here (instead)?
- –
-
How would you solve the problem?
- –
-
What would you like to see happen?
Per module: What are the specifics that should/must be added?
Appendix C. Guide for the Qualitative Interview
-
How would you lot depict your overall impression of the application?
-
Nursing documentation in general: What else would you like to see in the EMR regarding nursing documentation in the context of PPC?
- (a)
-
Is in that location anything that you felt was missing?
- (b)
-
Is there anything that yous did not feel was necessary?
- (c)
-
What other adjustments would y'all like to run into?
-
If not yet named: How did you find the service?
- (a)
-
Is there anything that you liked about it?
- (b)
-
Is there anything that you did not similar about it?
-
Tin can y'all depict in your ain words how y'all would charge per unit the clarity of the new modules: Was the content easy/quick to find?
-
If you imagine that the EMR/digital documentation were introduced in exercise for your unit:
- (a)
-
Tin can you draw for me in your own words what your fears would be if at that place was a switch from analogue to digital documentation?
- (b)
-
Can you describe to me in your own words what benefits you would hope to gain if there were a switch from analogue to digital documentation?
-
How did you experience near the test state of affairs?
- (a)
-
... especially the thinking out loud and the general state of affairs?
References
- Hoell, J.I.; Weber, H.; Warfsmann, J.; Trocan, 50.; Gagnon, G.; Danneberg, M.; Balzer, South.; Keller, T.; Janßen, G.; Kuhlen, M. Facing the Large Variety of Life-Limiting Atmospheric condition in Children. Eur. J. Pediatr. 2019, 178, 1893–1902. [Google Scholar] [CrossRef] [PubMed]
- Hoell, J.I.; Warfsmann, J.; Distelmaier, F.; Borkhardt, A.; Janßen, 1000.; Kuhlen, Grand. Challenges of Palliative Care in Children with Inborn Metabolic Diseases. Orphanet J. Rare Dis. 2018, xiii, 112. [Google Scholar] [CrossRef] [PubMed]
- Côté, A.-J.; Payot, A.; Gaucher, North. Paediatric Palliative Care in Practice: Perspectives between Astute and Long-Term Healthcare Teams. Acta Paediatr. 2019, 109, 613–619. [Google Scholar] [CrossRef] [PubMed]
- Connor, Due south.R.; Downing, J.; Marston, J. Estimating the Global Need for Palliative Care for Children: A Cross-Sectional Analysis. J. Pain Symptom Manag. 2016, 53, 171–177. [Google Scholar] [CrossRef]
- Trowbridge, A.; Stewart, Grand.T.; Rhee, E.; Hwang, J.Thousand. Providing Palliative Care in Rare Pediatric Diseases: A Case Serial of Three Children with Built Disorder of Glycosylation. J. Palliat. Med. 2017, 20, 104–106. [Google Scholar] [CrossRef]
- Thrane, S.E.; Maurer, S.H.; Cohen, S.M.; May, C.; Sereika, S.G. Pediatric Palliative Intendance: A Five-Twelvemonth Retrospective Chart Review Study. J. Palliat. Med. 2017, 20, 1104–1111. [Google Scholar] [CrossRef]
- Bender, H.U.; Riester, Yard.B.; Borasio, Chiliad.D.; Führer, One thousand. "Let's Bring Her Home First." Patient Characteristics and Identify of Death in Specialized Pediatric Palliative Home Care. J. Pain Symptom Manag. 2017, 54, 159–166. [Google Scholar] [CrossRef]
- Amarri, S.; Ottaviani, A.; Campagna, A.; De Panfilis, L. Children with Medical Complication and Paediatric Palliative Intendance: A Retrospective Cantankerous-Sectional Survey of Prevalence and Needs. Ital. J. Pediatr. 2021, 47, 110. [Google Scholar] [CrossRef]
- Nolte-Buchholtz, S.; Zernikow, B.; Wager, J. Pediatric Patients Receiving Specialized Palliative Home Care According to German language Constabulary: A Prospective Multicenter Cohort Study. Children 2018, v, 66. [Google Scholar] [CrossRef]
- Lin, Due south.-C.; Huang, One thousand.-C.; Yasmara, D.; Wuu, H.-Fifty. Impact of Palliative Care on End-of-Life care and Identify of Death in Children, Adolescents, and Immature Adults with Life-Limiting Conditions: A Systematic Review. Palliat. Support. Intendance 2021, xix, 488–500. [Google Scholar] [CrossRef]
- Kuo, D.Z.; McAllister, J.W.; Rossignol, L.; Turchi, R.G.; Stille, C.J. Intendance Coordination for Children with Medical Complexity: Whose Care Is It, Anyhow? Pediatrics 2018, 141, S224–S232. [Google Scholar] [CrossRef] [PubMed]
- Abebe, Eastward.; Scanlon, M.C.; Chen, H.; Yu, D. Complication of Documentation Needs for Children with Medical Complexity: Implications for Hospital Providers. Hosp. Pediatr. 2020, x, 00. [Google Scholar] [CrossRef] [PubMed]
- O'Donnell, H.C.; Suresh, South.; Webber, East.C.; Alexander, Yard.1000.; Chung, S.50.; Hamling, A.G.; Kirkendall, Due east.S.; Mann, A.M.; Sadeghian, R.; Shelov, E.; et al. Electronic Documentation in Pediatrics: The Rationale and Functionality Requirements. Pediatrics 2020, 146, 00. [Google Scholar] [CrossRef]
- Tsai, C.H.; Eghdam, A.; Davoody, N.; Wright, Yard.; Flowerday, S.; Koch, S. Furnishings of Electronic Wellness Tape Implementation and Barriers to Adoption and Use: A Scoping Review and Qualitative Analysis of the Content. Life 2020, 10, 327. [Google Scholar] [CrossRef]
- Rathert, C.; Porter, T.H.; Mittler, J.N.; Fleig-Palmer, Grand. Seven Years after Meaningful Apply: Physicians' and Nurses' Experiences with Electronic Wellness Records. Healthc. Manag. Rev. 2019, 44, 30–40. [Google Scholar] [CrossRef] [PubMed]
- Campanella, P.; Lovato, Due east.; Marone, C.; Fallacara, L.; Mancuso, A.; Ricciardi, West.; Specchia, K.L. The Bear on of Electronic Health Records on Healthcare Quality: A Systematic Review and Meta-Assay. Eur. J. Public Health 2015, 26, 60–64. [Google Scholar] [CrossRef]
- Akard, T.F.; Hendricks-Ferguson, V.Fifty.; Gilmer, M.J. Pediatric Palliative Care Nursing. Ann. Palliat. Med. 2019, viii, S39–S48. [Google Scholar] [CrossRef] [PubMed]
- Kaihlanen, A.-Chiliad.; Gluschkoff, G.; Hyppönen, H.; Kaipio, J.; Puttonen, S.; Vehko, T.; Saranto, K.; Karhe, L.; Heponiemi, T. The Associations of Electronic Health Record Usability and User Age with Stress and Cognitive Failures amid Finnish Registered Nurses: Cross-Exclusive Study. JMIR Med. Inform. 2020, eight, e23623. [Google Scholar] [CrossRef]
- Bøgeskov, B.O.; Grimshaw-Aagaard, Southward.L.S. Essential Task or Meaningless Burden? Nurses' Perceptions of the Value of Documentation. Nord. J. Nurs. Res. 2018, 39, ix–19. [Google Scholar] [CrossRef]
- Abu Raddaha, A.H.; Obeidat, A.; Al Awaisi, H.; Hayudini, J. Opinions, Perceptions and Attitudes toward an Electronic Health Tape Organisation among Practicing Nurses. J. Nurs. Educ. Pract. 2017, eight, 12. [Google Scholar] [CrossRef]
- Jedwab, R.; Hutchinson, A.; Manias, E.; Calvo, R.; Dobroff, N.; Glozier, N.; Redley, B. Nurse Motivation, Engagement and Well-Being before an Electronic Medical Record Organisation Implementation: A Mixed Methods Written report. Int. J. Environ. Res. Public Wellness 2021, 18, 2726. [Google Scholar] [CrossRef] [PubMed]
- Gephart, South.K.; Carrington, J.Yard.; Finley, B.A. A Systematic Review of Nurses' Experiences with Unintended Consequences When Using the Electronic Wellness Tape. Nurs. Adm. Q. 2015, 39, 345–356. [Google Scholar] [CrossRef] [PubMed]
- Powers, Eastward.Chiliad.; Shiffman, R.N.; Melnick, E.R.; Hickner, A.; Sharifi, M. Efficacy and Unintended Consequences of Hard-Stop Alerts in Electronic Health Record Systems: A Systematic Review. J. Am. Med. Inform. Assoc. 2018, 25, 1556–1566. [Google Scholar] [CrossRef] [PubMed]
- Snowden, A.; Kolb, H. Two Years of Unintended Consequences: Introducing an Electronic Health Record Arrangement in a Hospice in Scotland. J. Clin. Nurs. 2017, 26, 1414–1427. [Google Scholar] [CrossRef]
- Middleton, B.; Bloomrosen, M.; Dente, M.A.; Hashmat, B.; Koppel, R.; Overhage, J.; Payne, T.H.; Rosenbloom, S.T.; Weaver, C.; Zhang, J. Enhancing Patient Safe and Quality of Care by Improving the Usability of Electronic Health Record Systems: Recommendations from AMIA. J. Am. Med. Inform. Assoc. 2013, 20, e2–e8. [Google Scholar] [CrossRef]
- Kinnunen, U.-M.; Heponiemi, T.; Rajalahti, Due east.; Ahonen, O.; Korhonen, T.; Hyppönen, H. Factors Related to Health Informatics Competencies for Nurses—Results of a National Electronic Health Record Survey. CIN Comput. Inform. Nurs. 2019, 37, 420–429. [Google Scholar] [CrossRef]
- Salameh, B.; Boil, L.L.; Batran, A.; Hijaz, A.; Jaser, S. Nurses' Attitudes toward the Use of an Electronic Health Data System in a Developing Country. SAGE Open up Nurs. 2019, five, 2377960819843711. [Google Scholar] [CrossRef]
- Melnick, Due east.R.; West, C.P.; Nath, B.; Cipriano, P.F.; Peterson, C.; Satele, D.V.; Shanafelt, T.; Dyrbye, L.North. The Association between Perceived Electronic Wellness Record Usability and Professional Burnout amidst US Nurses. J. Am. Med. Inform. Assoc. 2021, 28, 1632–1641. [Google Scholar] [CrossRef]
- Khairat, South.; Xi, 50.; Liu, Southward.; Shrestha, S.; Austin, C. Understanding the Association between Electronic Health Record Satisfaction and the Well-Being of Nurses: Survey Study. JMIR Nurs. 2020, 3, e13996. [Google Scholar] [CrossRef]
- Harris, D.A.; Haskell, J.; Cooper, E.; Crouse, N.; Gardner, R. Estimating the Association betwixt Exhaustion and Electronic Wellness Record-Related Stress among Avant-garde Exercise Registered Nurses. Appl. Nurs. Res. 2018, 43, 36–41. [Google Scholar] [CrossRef]
- Khairat, S.; Coleman, G.C.; Ottmar, P.; Jayachander, D.I.; Bice, T.; Carson, S.S. Association of Electronic Health Record Use with Physician Fatigue and Efficiency. JAMA Netw. Open up 2020, iii, e207385. [Google Scholar] [CrossRef] [PubMed]
- Mazur, 50.1000.; Mosaly, P.R.; Moore, C.; Marks, L. Association of the Usability of Electronic Health Records with Cognitive Workload and Performance Levels amongst Physicians. JAMA Netw. Open 2019, ii, e191709. [Google Scholar] [CrossRef] [PubMed]
- Moore, G.; Wilding, H.; Gray, K.; Castle, D. Participatory Methods to Engage Wellness Service Users in the Development of Electronic Health Resources: Systematic Review. J. Particip. Med. 2019, xi, e11474. [Google Scholar] [CrossRef] [PubMed]
- Vandekerckhove, P.; de Mul, M.; Bramer, W.M.; de Bont, A.A. Generative Participatory Design Methodology to Develop Electronic Wellness Interventions: Systematic Literature Review. J. Med. Internet Res. 2020, 22, e13780. [Google Scholar] [CrossRef] [PubMed]
- Andargoli, A.E.; Scheepers, H.; Rajendran, D.; Sohal, A. Health Data Systems Evaluation Frameworks: A Systematic Review. Int. J. Med. Inform. 2017, 97, 195–209. [Google Scholar] [CrossRef]
- Vanderhook, S.; Abraham, J. Unintended Consequences of EHR Systems: A Narrative Review. In Proceedings of the International Symposium on Homo Factors and Ergonomics in Wellness Intendance, New Orleans, LA, The states, 5–8 March 2017; SAGE Publications: Los Angeles, CA, USA, 2017; Book 6, pp. 218–225. [Google Scholar] [CrossRef]
- Wisner, 1000.; Lyndon, A.; Chesla, C.A. The Electronic Health Record's Touch on Nurses' Cognitive Work: An Integrative Review. Int. J. Nurs. Stud. 2019, 94, 74–84. [Google Scholar] [CrossRef]
- Følstad, A. Users' Design Feedback in Usability Evaluation: A Literature Review. Human-Centric Comput. Inf. Sci. 2017, 7, xix. [Google Scholar] [CrossRef]
- Zurynski, Y.; Ellis, 50.A.; Tong, H.L.; Laranjo, Fifty.; Clay-Williams, R.; Testa, L.; Meulenbroeks, I.; Turton, C.; Sara, G. Implementation of Electronic Medical Records in Mental Health Settings: Scoping Review. JMIR Ment. Health 2021, 8, e30564. [Google Scholar] [CrossRef]
- Sadoughi, F.; Khodaveisi, T.; Ahmadi, H. The Used Theories for the Adoption of Electronic Wellness Tape: A Systematic Literature Review. Health Technol. 2018, 9, 383–400. [Google Scholar] [CrossRef]
- Venkatesh, V.; Morris, Chiliad.G.; Davis, M.B.; Davis, F.D. User Credence of Information Engineering science: Toward a Unified View. MIS Q. 2003, 27, 425–478. [Google Scholar] [CrossRef]
- Dabliz, R.; Poon, S.Grand.; Ritchie, A.; Burke, R.; Penm, J. Usability Evaluation of an Integrated Electronic Medication Management System Implemented in an Oncology Setting Using the Unified Theory of Acceptance and Use of Technology. BMC Med. Inform. Decis. Mak. 2021, 21, four. [Google Scholar] [CrossRef]
- Shiferaw, K.B.; Mehari, E.A. Modeling Predictors of Acceptance and Use of Electronic Medical Record System in a Resource Limited Setting: Using Modified UTAUT Model. Inform. Med. Unlocked 2019, 17, 100182. [Google Scholar] [CrossRef]
- Meyer, D.; Kernebeck, South.; Busse, T.; Ehlers, J.; Wager, J.; Zernikow, B.; Dreier, Fifty. Electronic Health Records in Specialized Pediatric Palliative Intendance: A Qualitative Needs Assessment among Professionals Experienced and Inexperienced in Electronic Documentation. Children 2021, 8, 249. [Google Scholar] [CrossRef] [PubMed]
- Kernebeck, S.; Busse, T.Due south.; Jux, C.; Meyer, D.; Dreier, L.A.; Zenz, D.; Zernikow, B.; Ehlers, J.P. Participatory Blueprint of an Electronic Medical Record for Paediatric Palliative Intendance: A Retrieve-Aloud Report with Nurses and Physicians. Children 2021, 8, 695. [Google Scholar] [CrossRef] [PubMed]
- Fan, One thousand.; Lin, J.; Chung, C.; Truong, K.North. Concurrent Call up-Aloud Verbalizations and Usability Problems. ACM Trans. Comput. Interact. 2019, 26, 1–35. [Google Scholar] [CrossRef]
- Alhadreti, O. Comparing Two Methods of Usability Testing in Saudi Arabia: Concurrent Think-Aloud vs. Co-Discovery. Int. J. Hum.-Comput. Collaborate. 2020, 37, 118–130. [Google Scholar] [CrossRef]
- Roman, Fifty.C.; Ancker, J.S.; Johnson, South.B.; Senathirajah, Y. Navigation in the Electronic Health Record: A Review of the Rubber and Usability Literature. J. Biomed. Inform. 2017, 67, 69–79. [Google Scholar] [CrossRef]
- McDonald, Southward.; Edwards, H.M.; Zhao, T. Exploring Recollect-Alouds in Usability Testing: An International Survey. IEEE Trans. Undecayed Secur. Comput. 2012, 55, two–19. [Google Scholar] [CrossRef]
- Busse, T.S.; Jux, C.; Kernebeck, Southward.; Dreier, L.A.; Meyer, D.; Zenz, D.; Zernikow, B.; Ehlers, J.P. Participatory Pattern of an Electronic Cross-Facility Health Record (ECHR) Organisation for Pediatric Palliative Care: A Think-Aloud Study. Children 2021, 8, 839. [Google Scholar] [CrossRef]
- Russ, A.Fifty.; Saleem, J.J. Ten factors to consider when developing usability scenarios and tasks for wellness information technology. J. Biomed. Inform. 2018, 78, 123–133. [Google Scholar] [CrossRef]
- Dresing, T.; Pehl, T. Praxisbuch Interview, Transkription & Analyse. Anleitungen und Regelsysteme für Qualitativ Forschende; Eigenverlag: Marburg, Germany, 2018. [Google Scholar]
- O'Malley, A.Due south.; Draper, K.; Gourevitch, R.; Cross, D.A.; Scholle, S.H. Electronic Wellness Records and Support for Primary Care Teamwork. J. Am. Med. Inform. Assoc. 2015, 22, 426–434. [Google Scholar] [CrossRef] [PubMed]
- Arndt, B.G.; Beasley, J.W.; Watkinson, M.D.; Temte, J.L.; Tuan, W.-J.; Sinsky, C.A.; Gilchrist, V.J. Tethered to the EHR: Primary Care Physician Workload Assessment Using EHR Result Log Data and Fourth dimension-Motility Observations. Ann. Fam. Med. 2017, 15, 419–426. [Google Scholar] [CrossRef] [PubMed]
- Potato, D.R.; Giardina, T.D.; Satterly, T.; Sittig, D.F.; Singh, H. An Exploration of Barriers, Facilitators, and Suggestions for Improving Electronic Health Record Inbox-Related Usability. JAMA Netw. Open 2019, 2, e1912638. [Google Scholar] [CrossRef] [PubMed]
- Tai-Seale, M.; Dillon, E.C.; Yang, Y.; Nordgren, R.; Steinberg, R.50.; Nauenberg, T.; Lee, T.C.; Meehan, A.; Li, J.; Chan, A.S.; et al. Physicians' Well-Being Linked to In-Basket Messages Generated by Algorithms In Electronic Health Records. Health Aff. 2019, 38, 1073–1078. [Google Scholar] [CrossRef]
- Farokhzadian, J.; Khajouei, R.; Hasman, A.; Ahmadian, L. Nurses' Experiences and Viewpoints virtually the Benefits of Adopting Information technology in Health Care: A Qualitative Study in Islamic republic of iran. BMC Med. Inform. Decis. Mak. 2020, 20, 240. [Google Scholar] [CrossRef] [PubMed]
- Kossman, S.P.; Scheidenhelm, S.L. Nurses' Perceptions of the Bear upon of Electronic Health Records on Piece of work and Patient Outcomes. CIN Comput. Inform. Nurs. 2008, 26, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, L.; Bellucci, E.; Nguyen, L.T. Electronic Wellness Records Implementation: An Evaluation of Data System Affect and Contingency Factors. Int. J. Med. Inform. 2014, 83, 779–796. [Google Scholar] [CrossRef]
- Pollack, A.H.; Pratt, West. Association of Health Tape Visualizations with Physicians' Cognitive Load When Prioritizing Hospitalized Patients. JAMA Netw. Open 2020, 3, e1919301. [Google Scholar] [CrossRef]
- De Leeuw, J.A.; Woltjer, H.; Kool, R.B. Identification of Factors Influencing the Adoption of Health Data Engineering by Nurses Who Are Digitally Lagging: In-Depth Interview Report. J. Med. Internet Res. 2020, 22, e15630. [Google Scholar] [CrossRef]
- Wiebe, North.; Varela, Fifty.O.; Niven, D.J.; Ronksley, P.E.; Iragorri, North.; Quan, H. Evaluation of Interventions to Amend Inpatient Hospital Documentation within Electronic Health Records: A Systematic Review. J. Am. Med. Inform. Assoc. 2019, 26, 1389–1400. [Google Scholar] [CrossRef]
- Schaaf, J.; Sedlmayr, M.; Sedlmayr, B.; Prokosch, H.-U.; Storf, H. Evaluation of a Clinical Decision Support System for Rare Diseases: A Qualitative Study. BMC Med. Inform. Decis. Mak. 2021, 21, 65. [Google Scholar] [CrossRef] [PubMed]
- Alroobaea, R.; Mayhew, P.J. How Many Participants Are Actually Enough for Usability Studies? In Proceedings of the Science and Information Conference, London, UK, 27–29 August 2014; pp. 48–56. [Google Scholar] [CrossRef]
- Aiyegbusi, O.L. Fundamental methodological considerations for usability testing of electronic patient-reported result (ePRO) systems. Qual. Life Res. 2020, 29, 325–333. [Google Scholar] [CrossRef] [PubMed]
- Peute, L.W.; de Keizer, N.F.; Jaspers, Grand.Due west. The Value of Retrospective and Concurrent Call up Aloud in Formative Usability Testing of a Medico Data Query Tool. J. Biomed. Inform. 2015, 55, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Prokop, M.; Pilař, 50.; Tichá, I. Impact of Think-Aloud on Center-Tracking: A Comparison of Concurrent and Retrospective Think-Aloud for Research on Controlling in the Game Surround. Sensors 2020, 20, 2750. [Google Scholar] [CrossRef]
- Richardson, S.; Mishuris, R.; O'Connell, A.; Feldstein, D.; Hess, R.; Smith, P.; McCullagh, L.; McGinn, T.; Mann, D. "Recollect Aloud" and "Near Live" Usability Testing of 2 Complex Clinical Decision Support Tools. Int. J. Med. Inform. 2017, 106, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Bergen, Northward.; Labonté, R. "Everything Is Perfect, and We Accept No Problems": Detecting and Limiting Social Desirability Bias in Qualitative Research. Qual. Health Res. 2019, thirty, 783–792. [Google Scholar] [CrossRef]
- Bansler, J.P. Challenges in User-Driven Optimization of EHR: A Instance Written report of a Large Epic Implementation in Denmark. Int. J. Med. Inform. 2021, 148, 104394. [Google Scholar] [CrossRef]
- Moon, M.C.; Hills, R.; Demiris, Yard. Understanding Optimisation Processes of Electronic Health Records (EHRs) in Select Leading Hospitals: A Qualitative Study. BMJ Healthc. Inform. 2018, 25, 109–125. [Google Scholar] [CrossRef]
- Skela-Savič, B.; Lobe, B. Differences in Beliefs on and Implementation of Evidence-Based Do According to Blazon of Health Care Institution—A National Cantankerous-Exclusive Study among Slovenian Nurses. J. Nurs. Manag. 2020, 29, 971–981. [Google Scholar] [CrossRef]
Figure 1. Overview of the characteristics of components for the nursing documentation module. (Icons made by Freepik from www.flaticon.com, accessed on 28 November 2021).
Effigy 1. Overview of the characteristics of components for the nursing documentation module. (Icons fabricated by Freepik from www.flaticon.com, accessed on 28 November 2021).
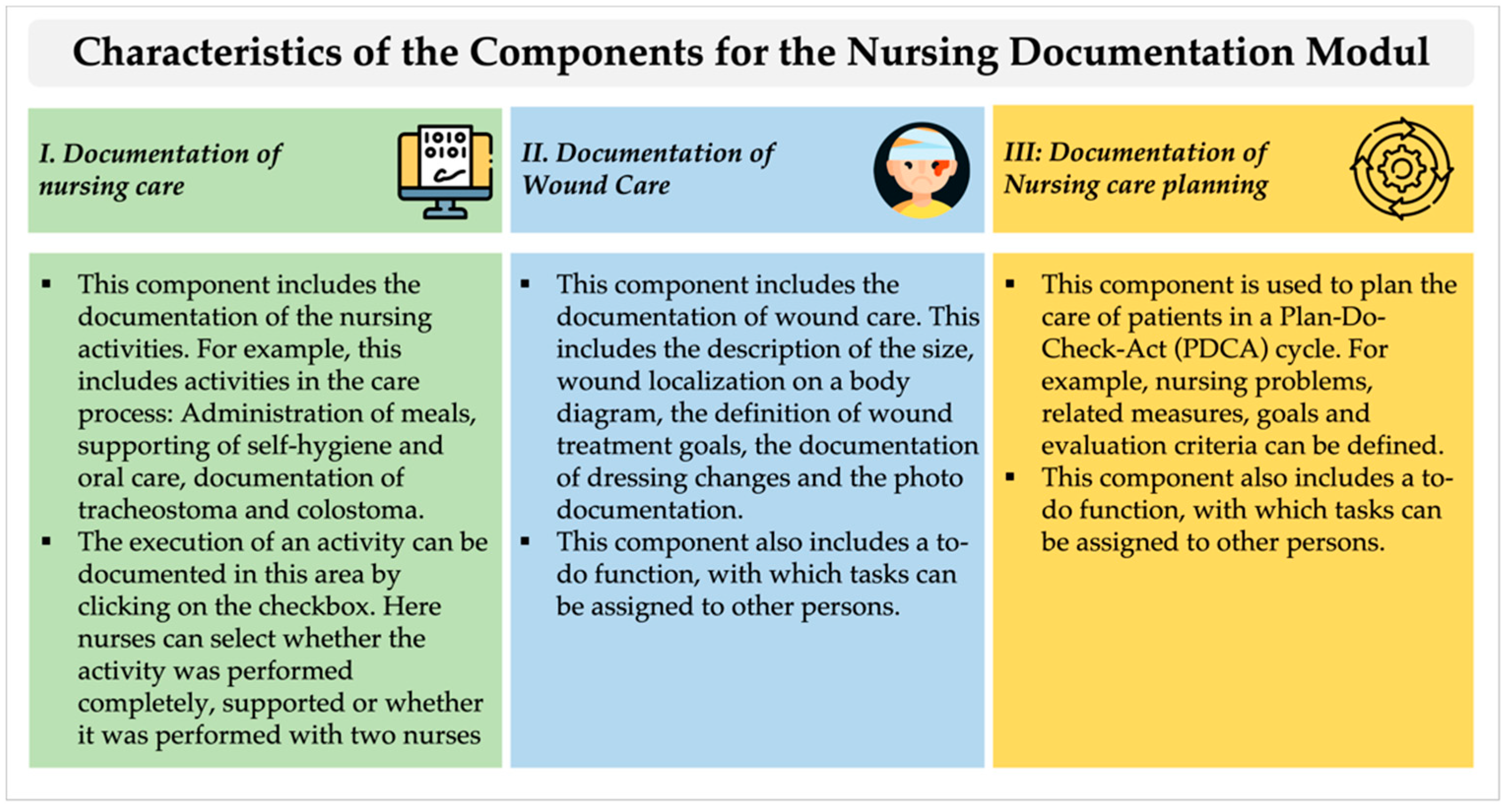
Figure 2. Overview of the primary categories and subcategories based on UTAUT.
Figure 2. Overview of the main categories and subcategories based on UTAUT.

Effigy 3. Documentation of the component for documenting nursing activities.
Figure iii. Documentation of the component for documenting nursing activities.

Figure 4. Mouseover field for documenting nursing activities in the patient chart view.
Figure 4. Mouseover field for documenting nursing activities in the patient nautical chart view.
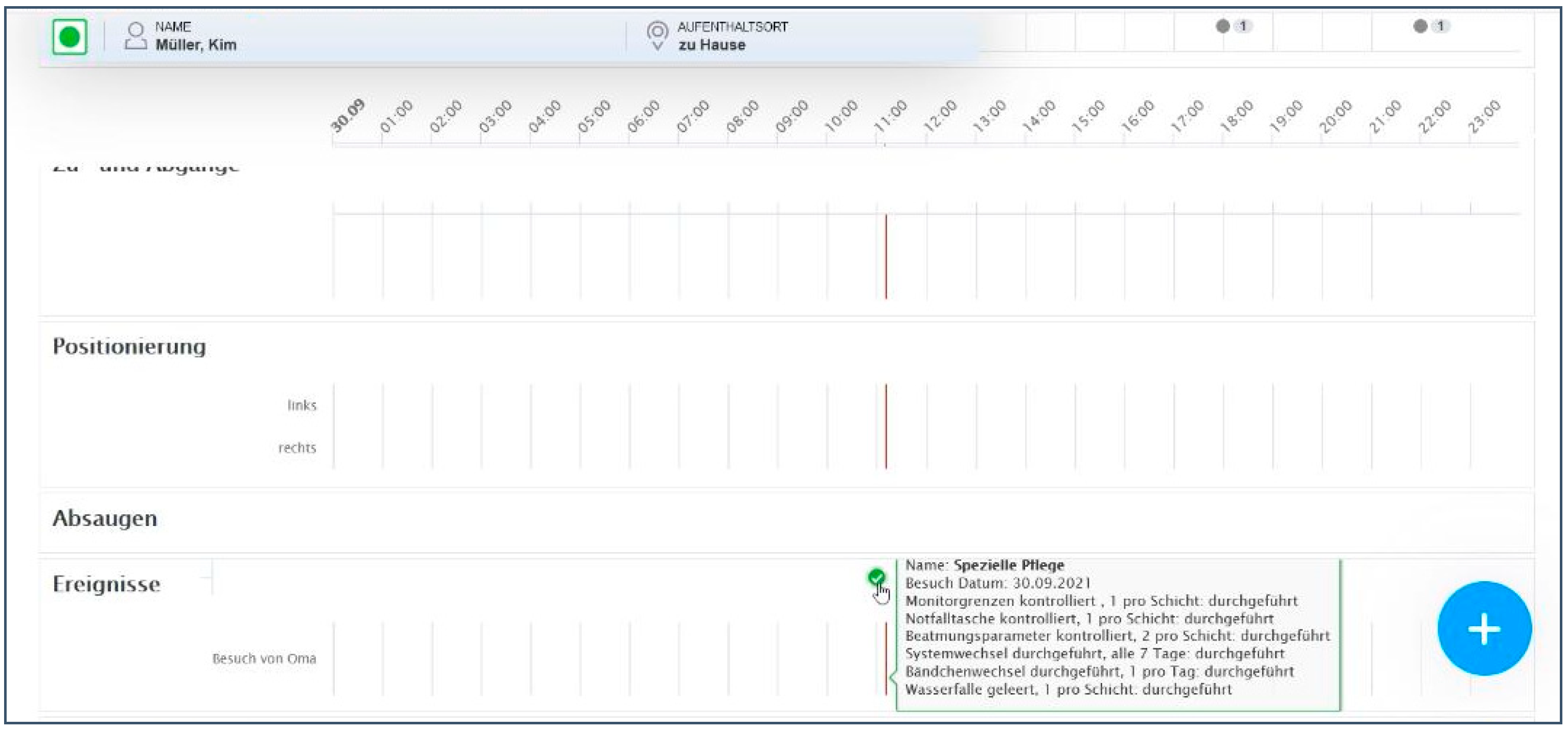
Table 1. Definitions of the core direct determinants of UTAUT [41].
Table 1. Definitions of the core direct determinants of UTAUT [41].
| UTAUT Determinant | Definition |
|---|---|
| Performance expectancy | "The degree to which an individual believes that using the system volition aid him or her to achieve gains in job functioning," which encompasses mainly the functionalities of a technology. |
| Effort expectancy | "The degree of ease associated with the use of the system," which basically includes the dimension of perceived usability and complexity of use. |
| Social influence | "The degree to which an individual perceives that important others believe he or she should utilise the new system". |
| Facilitating conditions | "The degree to which an individual believes that an organizational and technical infrastructure exists to support use of the system". |
Tabular array two. Overview of participant characteristics.
Table 2. Overview of participant characteristics.
| Characteristic | due north (%) |
|---|---|
| Sex | |
| Female | 11 |
| Male person | 0 |
| Age in years (Mean) | 36 one |
| Profession | |
| Nurse | 11 1 |
| Years of PPC experience | |
| 0–9 | 3 1 |
| x–xx | 4 one |
| >20 | ii i |
| Years of experience in current position | |
| 0–9 | iv 1 |
| ten–20 | 4 1 |
| >xx | 1 1 |
| Feel in professional employ of EMR | 0 1 |
| Publisher'due south Notation: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open admission article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/past/4.0/).
easterlinghosturnelf.blogspot.com
Source: https://www.mdpi.com/1660-4601/19/6/3637/htm
0 Response to "Unit 6 Study Guide Review Module 15 Surface Area and Volume of Solids Answer Key"
Post a Comment